Specializing in precision microsurgery to restore hearing,
treat chronic infections, and resolve complex middle ear disorders.
Clinical Indication: Persistent Otitis Media with Effusion (Glue Ear), which doesn't resolve with medication, or barotrauma from frequent flying.
The Procedure: Using high-magnification microscopy, a microscopic incision is made in the tympanic membrane. A tiny ventilation tube (Grommet) is inserted to equalize pressure between the outer and middle ear.
Recovery: Most patients return to normal activities within 24 hours. The tubes usually fall out naturally within 6 to 12 months as the eardrum heals.
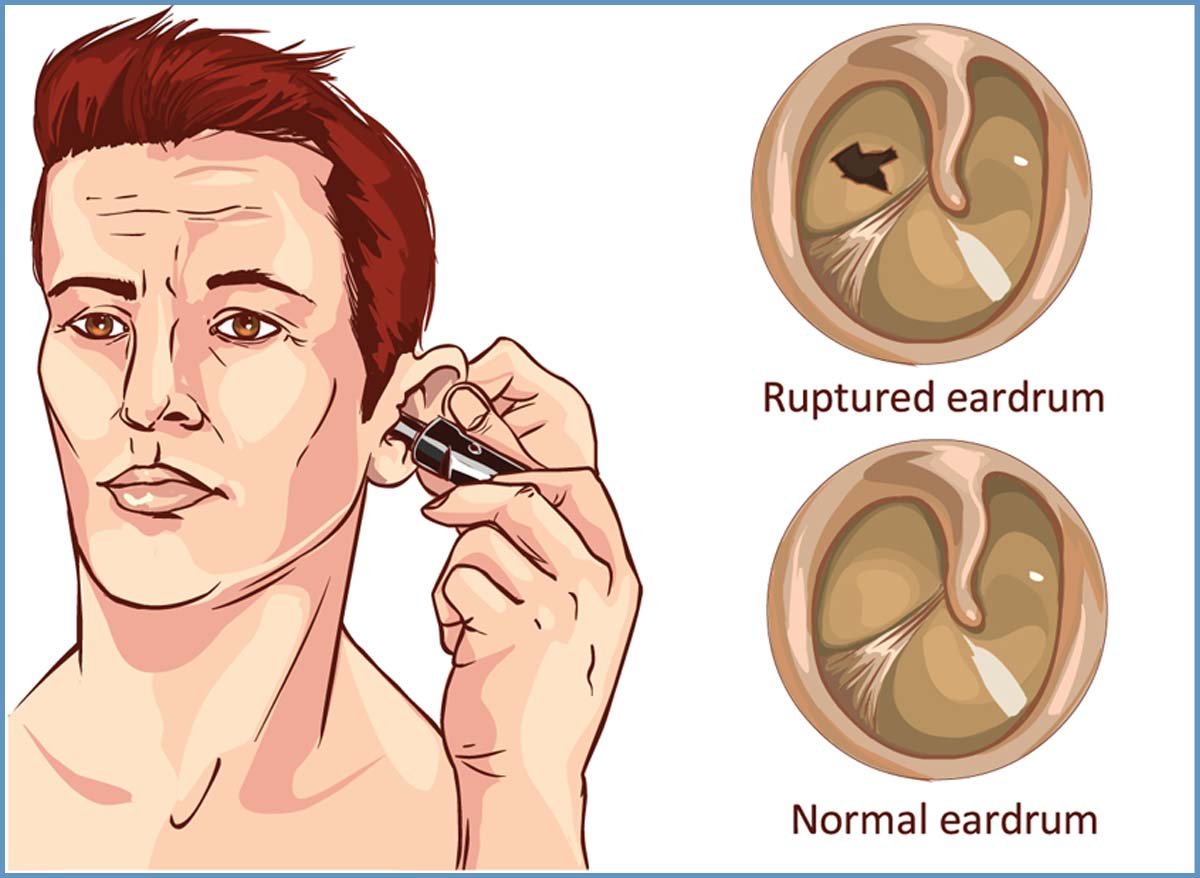
Clinical Indication: Perforated eardrums caused by trauma, loud blasts, or chronic infections that cause intermittent discharge and hearing loss.
The Procedure: We utilize modern Underlay or Overlay grafting techniques. A small piece of fascia (connective tissue) or cartilage is harvested from behind the ear to act as a permanent patch for the hole.
The Goal: To create a "dry ear," prevent bacteria from entering the middle ear space, and improve the vibratory capacity of the drum for better hearing.
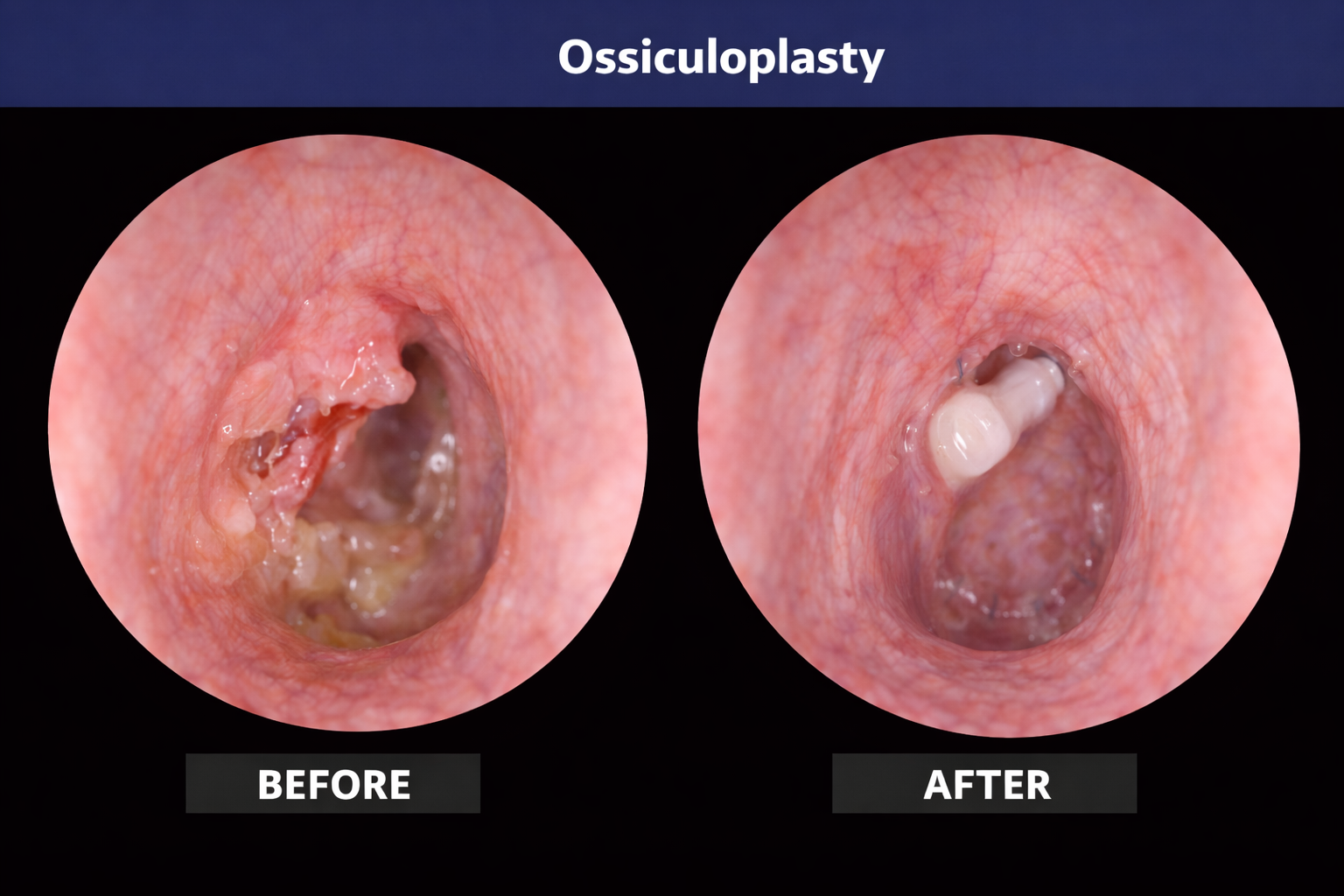
Clinical Indication: Discontinuity or erosion of the ossicular chain (the tiny bones: Malleus, Incus, Stapes) often due to chronic disease.
The Procedure: This delicate microsurgery replaces damaged bones with either PORP (Partial Ossicular Replacement Prosthesis) or TORP (Total Ossicular Replacement Prosthesis) made of biocompatible Titanium or Teflon.
Outcome: Significant restoration of the mechanical sound transmission from the eardrum to the inner ear, reducing the "Air-Bone Gap" in hearing tests.
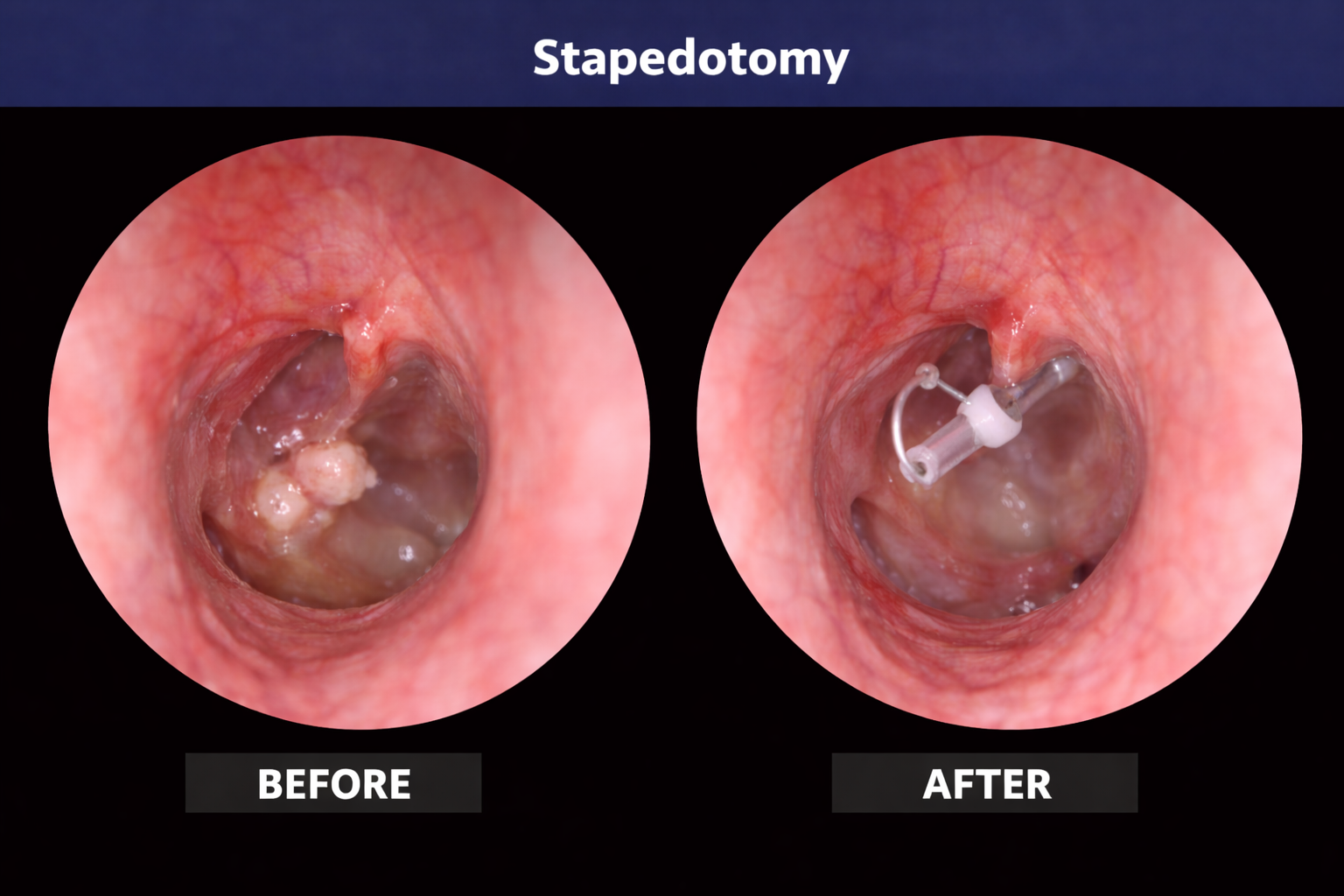
Clinical Indication: Otosclerosis, a condition where the stapes bone becomes "fixed" and cannot vibrate, leading to progressive hearing loss.
The Procedure: A laser or micro-drill is used to create a tiny hole in the footplate of the stapes. A micro-piston is then placed to bypass the fixed bone and restore fluid motion in the inner ear.
Patient Note: This is a highly specialized surgery that often results in a "dramatic" improvement in hearing immediately or shortly after the healing phase.
"Modern stapedotomy has largely replaced the older stapedectomy, offering safer results and faster recovery for patients with bone-fixation hearing loss."
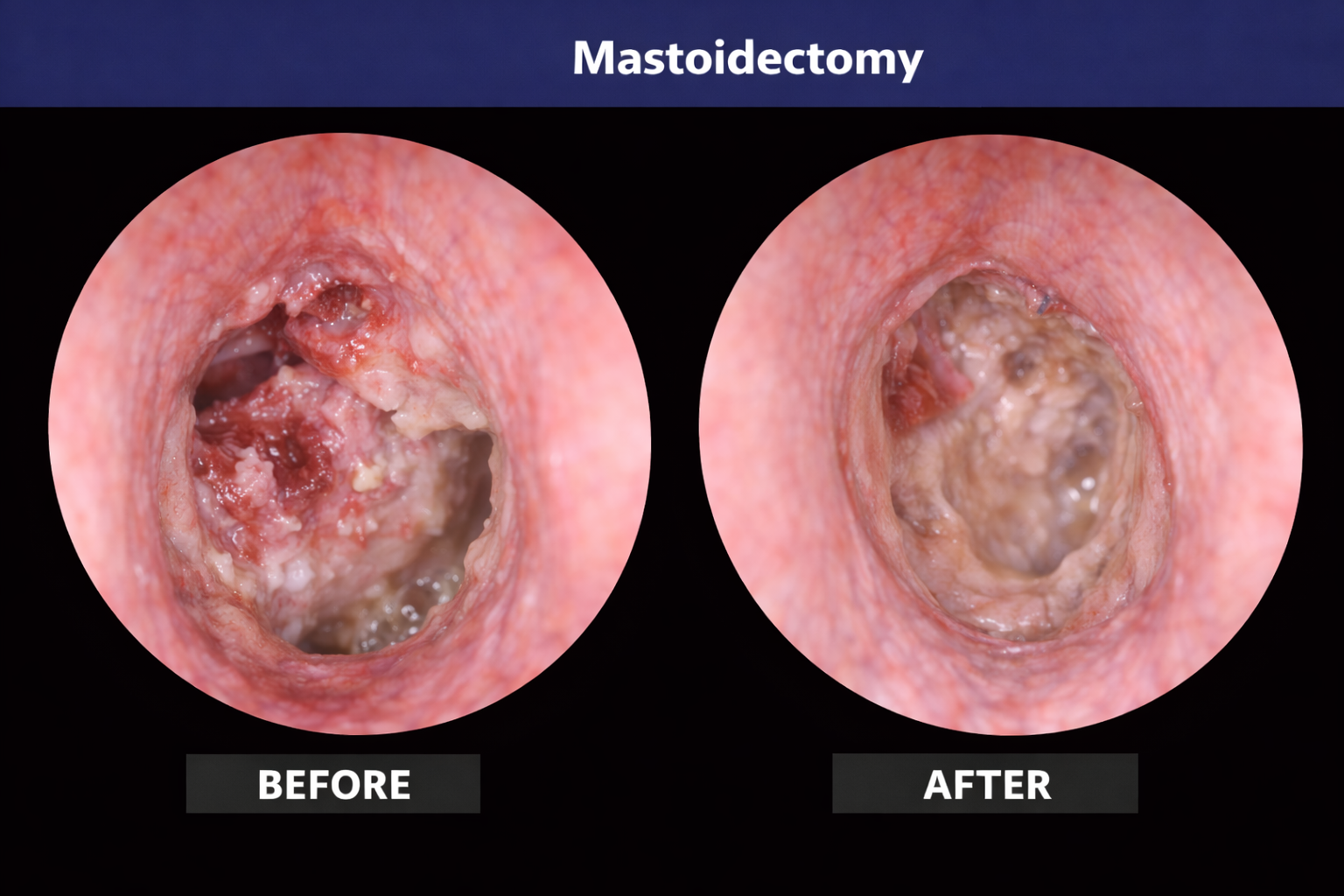
Clinical Indication: Chronic Suppurative Otitis Media (CSOM) or Cholesteatoma—a non-cancerous but destructive skin cyst that eats through ear bone.
The Procedure: We perform either a Canal Wall Down (CWD) or Canal Wall Up (CWU) mastoidectomy to drill away infected bone and clear the mastoid air cells.
Safety First: Our surgeons use advanced facial nerve monitoring during this procedure to ensure the nerves controlling your facial expressions are fully protected.
Advanced technology to ensure zero nerve damage during bone drilling.